|
|
Postural
syndroms
Relationship between temporomandibular disorders and
posture
Mauro
Lastrico T.d R.
|
Introductory
notes:
1) The TMJ is a convex-concave and concave-convex joint between
mandibular condyle, disk and temporal bone.
2) The muscles called "masticatory muscles" acting upon this joint
are the masseter, the temporalis, the medial and lateral pterygoid.
3) In functional terms, these muscles bestow stability to the
joint and permit to fit the teeth together (to close the mouth).
4) Though being monoarticular muscles, they can interact with
the whole skeletal muscle architecture.
The physical laws governing complex systems have shown that whenever
several forces are acting upon a system (skeletal bones), these
forces are joint and interacting with each other. 5. (Correct)
posture means a correct skeletal sequence of articulations, irrespective
of the spatial position of the body .
The
physiology of deglution
Swallowing is an unvoluntary reflex movement which is evoked several
times per minute; to enable us to swallow, the muscles of mastication
contract and make our teeth come in contact.
If dentition is physiologically correct, the masticatory muscles
have the same intensity of action, since they utilize the minimum
bite force required. The bite shall be such as not to affect other
body areas, that is to say following a physiological pattern.
No relationship between temporomandibular joint and posture will
result.
Relation
between temporomandibular joint and posture
Physiologically, there should be no relation between temporomandibular
joint and posture; nevertheless, this connection will occur if
dentition is pathologically positioned in the dental arch. Three
events may be more frequently observed, namely:
a) teeth of different length (pre-contact)
b) excessive freeway space
c) reduction or absence of freeway space
Teeth of different length (pre-contact) If the teeth in a dental
arch are too long or too short, the masticatory muscles will function
asymmetrically (right-left) and with more intensity than physiologically
required when closing the mouth. The first result will be that
the condyle of the temporalis on the side of the "short" teeth
will extend beyond its physiological position towards the mandibular
fossa to allow teeth contact. The mandible will then make a twisting
movement. This event may trigger painful symptoms especially affecting
the TMJ, the ear and the head, since many receptors are located
inside the mandibular fossa. Furthermore, with reference to the
statements made in para. 4 of the introduction, an asymmetric
and excessively intense activation of muscles will involve other
muscle regions, starting from the muscles of the neck. Overstraining
or tension of the muscles will not be restricted to the masticatory
muscles, but other joints, too, will be subject to the traction
force of the muscles, the cervical vertebrae will lose their symmetric
position, which may also result in a raised shoulder and involve
a variety of complex skeletal alterations if this pathological
issue should perpetuate over time. .
The result will be an altered body posture.
Excessive
freeway space
At rest, that is to say when the muscles of mastication are relaxed,
the teeth should not fit together but show an about 2-mm "freeway
space".
This is considered by our brain circuits as the proper physiological
rest condition.
In case of excessive freeway space, for example because of generally
"too short" teeth, the muscles of mastication should be constantly
tense to maintain a correct freeway space. To counterbalance this
continuous fatigue, the muscle system and particularly the muscles
positioned anteriorly to the cervical spine, inserting into the
third thoracic vertebrae, will cause the whole head to move forward.
The dental arches will then meet and unload the overwork of the
masticatory muscles.
However, a forward displacement of the head also means displacement
of the barycentre of the body. To prevent us from losing our balance,
the underlying muscle zones will be activated by modifying the
pattern of the whole vertebral spine, thus accentuating or reducing
physiological lordoses and resulting in an altered vertical sequence
of the body segments.
In this case, too, the result will be a postural alteration.
Reduction or absence of freeway space
This problem is opposite to the foregoing.
In this case, the post-cervical group of muscles will be activated
so as to draw the head back. The dental arches will then be slightly
apart, thus unloading the work of the hyoid muscles. Again, the
barycentre of the body will be displaced this time posteriorly
and the underlying musculature must be activated to keep the balance
by acting on the whole spine, which will lead to an altered vertical
sequence of the body segments.
The result will be an altered posture.
All postural disorders taken into examination may cause, in turn,
orthopedic pathologies (e.g. scoliosis, lumbago, cervicodynia,
etc), that may be defined as subsequent to a primary pathologic
involvement of the buccal system .
|
|
|
|
Relation
between posture and temporomandibular joint
The mechanisms previously discussed may also act inversely, i.e.
a muscular unbalance originated from other body zones may trigger
TMJ disorders caused by interconnected muscle systems.
Our muscle system as a whole may suffer primary (system-inborne)
or secondary shortening processes (resulting from other malfunctioning
structures). In both cases the issue will be postural problems in
the long run.
|
|
|
|
|
 |
Diagnosis
Posture is a complex, multifactorial problem, that is to say it
can be altered by numerous systems (e.g. masticatory, visual, auditive,
neurological, musculoskeletal systems, etc.), including the emotional
background. It is up to the posturologist to make a differential
diagnosis in co-operation with various specialists to find both
a causal and a symptomatological solution to the problem under examination.
In the specific TMJ case, which is one of the joints most often
involved in postural disorders, the co-operation of the dentist-posturologist
with a therapist-posturologist is imperative to conduct first a
differential diagnosis test and then to study the best therapeutic
approach.
|
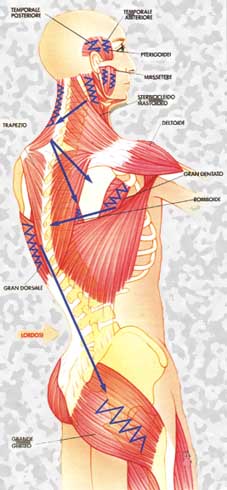
Tipical
muscular contraction and postural disorders starting from unbalanced
bite
(Cignetti) |
|
Self-testing
Some symptoms may be predictive of skeletal and postural problems
caused by the temporomandibular joint, like:
-
ear pain (in absence of ORL problems)
- joint
clicks and difficulty in opening and/or closing the mouth
-
headache
-
cervicobrachialgia
-
lumbar and/or dorsal aches (with head bent in forward or backward
position).
A
posturologic examination is always recommended if any of the above
symptoms is reported.
|
|
Treatment
Whenever the differential diagnosis suggests that there is a postural
problem caused by TMJ, the first approach must be made by the dentist
with the use of a bite or an orthotic appliance. These (mobile)
appliances preferably positioned on the lower dental arch are designed
to restore a correct dental occlusion allowing correct swallowing
and, therefore, a correct TMJ posture. Afterwards, when the system
is stabilized, it should be assessed whether a permanent action
on the teeth is appropriate.
Between a bite and orthotic option, the latter is preferable because
of its accuracy and characteristic of reproducing an optimum dentition.
To utilize this appliance, it is however imperative for the dentist
to use the kinesiograph, a complex instrument allowing to mold the
orthotic appliance while respecting the physiological pattern.
During the treatment period with the mobile appliance, it should
be assessed whether a physiotherapeutic treatment should be associated
to solve any residual shortening of the muscles.
Conversely, when the differential diagnosis shows a TMJ disorder
resulting from postural unbalance, the first approach must be made
by the therapist-posturologist who shall re-balance (stretching)
the muscle forces acting on the skeletal system so as to restore
the correct physiological posture of all joints.
The techniques most often utilized for this purpose are the Mézières,
RPG and Rolfing Methods. The option for treatment by a dentist with
the above-described appliances can be considered only afterwards,
when the musculoskeletal system has gained sufficient stabilization.
.
|
|
|
|
|
|
|